Breast enlargement
The breast plays a key role in shaping the front body contours and determining femininity. The ideal breast is a cone- or hemispherical formula with its base on the chest wall, the most prominent point being the bud. It does not exceed the front snowline on the side and its internal boundaries are between 3 cm and 4 cm apart. A straight line imagined through the buds, i.e. equally convex and convex above and below the breast axis, is mass. At the end of sexual maturation, the female breast becomes enlarged and hemispherical, for which the fat layer, capsula adiposa, is primarily responsible, because the glands, parenchyma, develop during pregnancy, are the largest at the time of milk weaning, and then develop back to their original size from the end of breastfeeding. If the normal development and growth of the breast in the puberty age is not possible, we speak of poorly developed hypoplasia or missing aplastic breasts. At a later stage in life, the breast-feeding population may decrease significantly after significant decline. Today’s behavioural changes and media-mediated beauty ideals play a decisive role in shaping what is considered to be an ‘ideal’ form. Smaller messes often cause psychic problems in everyday life, in work placements, dressing and socialising. Problems can be corrected well by silicone implantation. The implants developed in the mid-1960s are in fact silicone flexible bags filled with silicone gel. The implants are filled with silicone polymers of various densities (cohesivities). Silicone is a chain polymer (macrolecule) containing polydimethylsiloxane, i.e. siloxane (-Si-O-Si) bonds. The density (cohesivitation) of the gel is determined by the number of organic groups of methyl (-CH3). In the case of two methyl groups, if the chain is short, silicone oil, if the polymer chain is larger, a thick plastic silicone material may be produced.
Silicone is a widely used and accepted substance in medicine. In paediatric surgery, it was used for the first time (1950) in children with waterheads to drain intracranial fluid. Commonly used and used in cardiac surgery, urology, neurosurgery, ophthalmology (tracheotomy tube, lens of the eye, cardiac valve, coating of hypoderm needles, developmental disorder, or reconstruction implants used in tumour surgery).
The use of silicone has given rise to a lot of debate about its potential harmful effects on the organism. Sensationalist press articles and reports by the media, listing burns, referred to breast implants containing silicone implants as timed bombs.
The EQUAM (European Comittee on Quality Assurance and Medical Devices in Plastic Surgery), issued on 23 June 200, states that silicone does not have any harmful effects on health. There is no scientific evidence of its effects on carcinogenic, musculoskeletal, autoimmune or connective tissue diseases. Silicone gel implants do not adversely affect pregnancy, foetal development, breastfeeding or the health of breast-fed children.
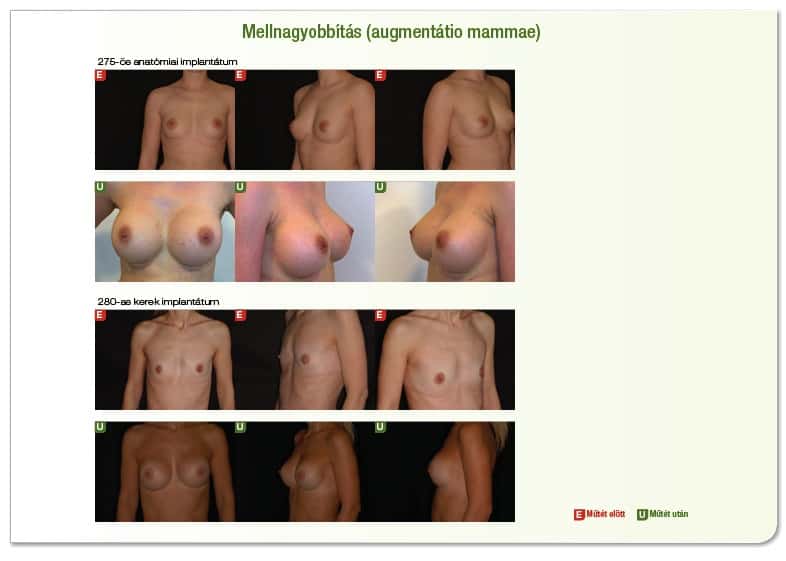
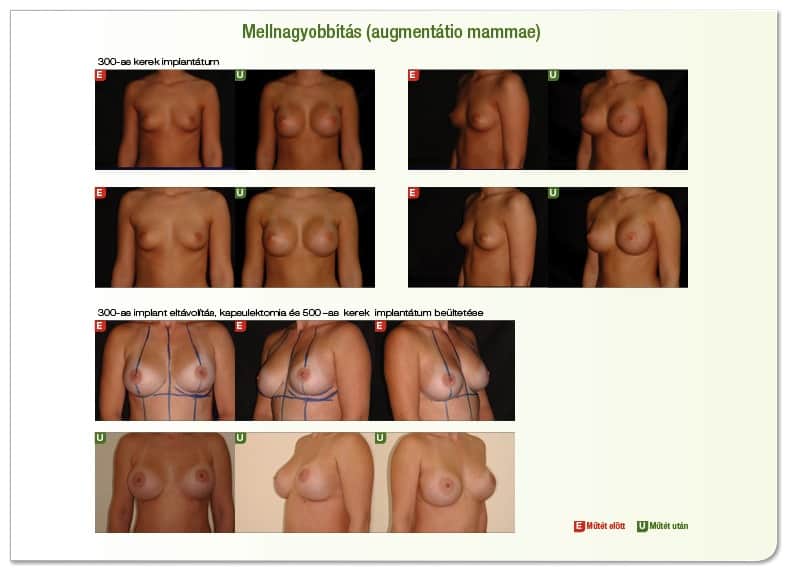
The implants used are always selected according to the individual’s morphology, existing breast form, chest shape, possible deformation and patient wishes after prior discussion and consultation. Selection is determined by the basis of the existing breast, loose skin, amount of breast tissue, patient expectations, surgical limits and possibilities, aesthetics and asymmetry.
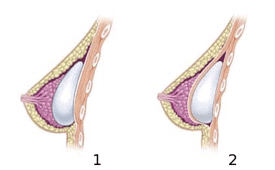
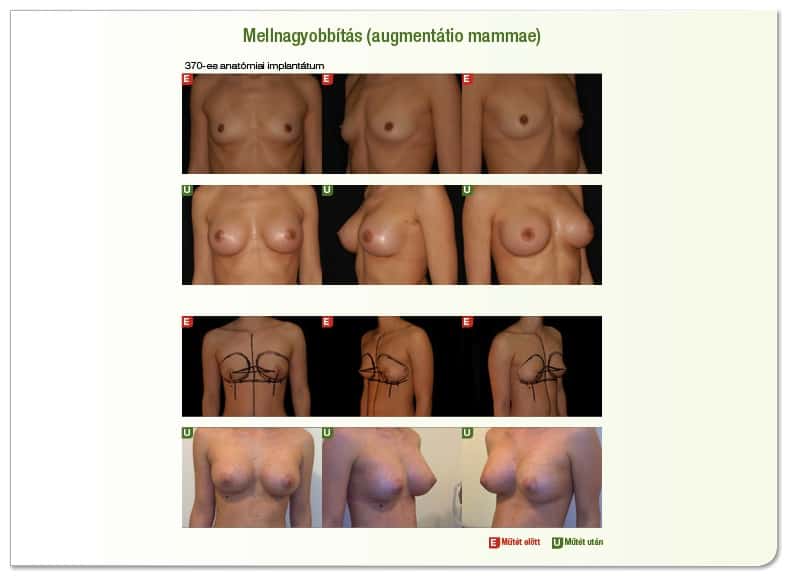
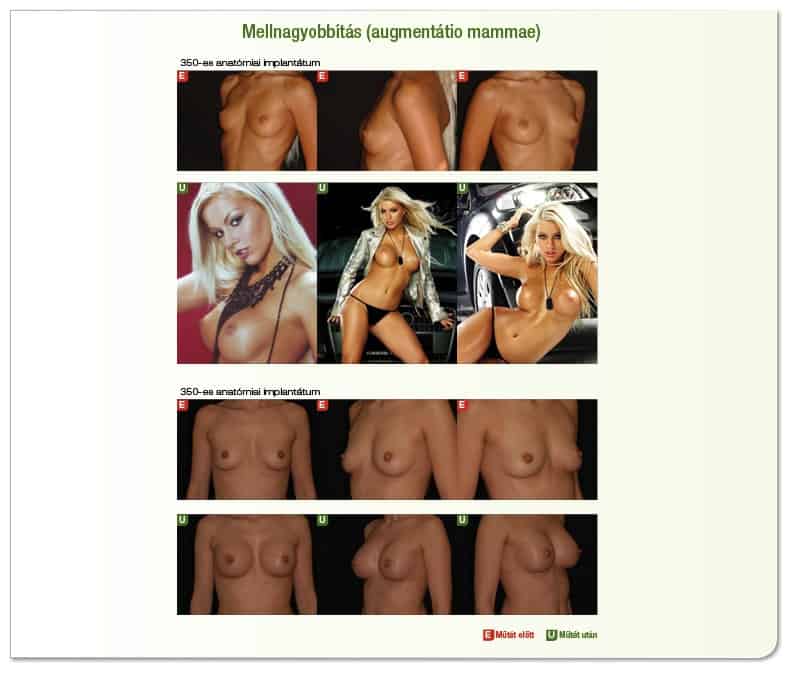
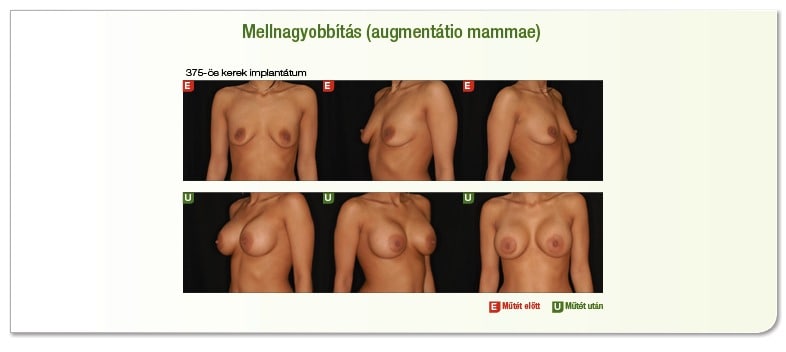
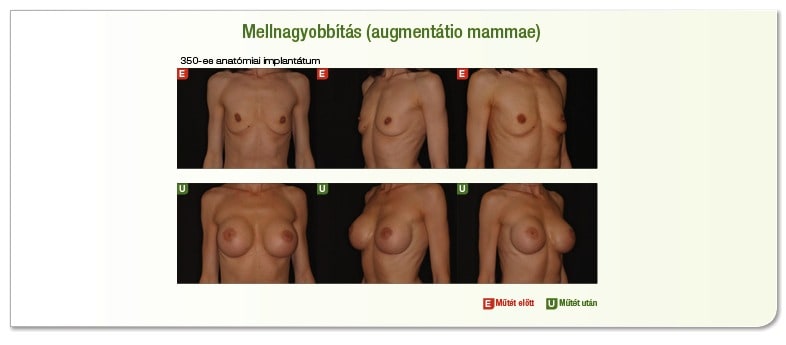
The implant may be round or anatomical in shape, also known as droplets. Smooth (standard) rough (textured) surface, low, medium, high or extra high profile. Rather, the form of the anatomy is characterised by the fact that the new breast formed is more natural, less prominent and does not appear to have been enriched with an implant.
Surgery after a preliminary examination, including routine laboratory tests, ECG, MRTG depending on age, or breast tests (ultrasound or mammographia).
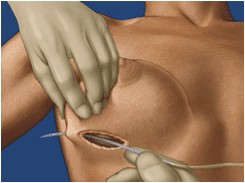
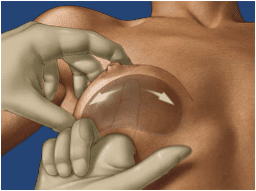
Surgery is carried out in anaesthesia. The operation consists of inserting a silicone implant behind the breast stock.
Intrusions can occur at several locations: the inframammaris, the peri-circular incision at the lower edge of the bud yard and theaxillaris incision in the snow.
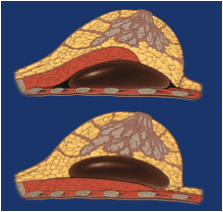
The implant can be placed directly behind the mammary gland (subglandularis), i.e. between the mammary gland and the thoracic muscle, behind the thoracic muscle (submuscularis), i.e. between the thoracic muscle and the thoracic wall, or in combination with the “dual plane” method, when the lower half of the implant is below the breast stock and the upper half below the thoracic muscle.
The advantage of placing the implant under the gland population is that the duration of the operation is shorter, the operation is easier to perform, and there is less pain and discomfort in the post-operative period. Surgery for implantation behind the breast muscle is technically more difficult, the duration of the operation is longer and more pronounced pain is seen during the post-operational period, but the number of late complications is smaller, the implant is less noticeable, visible, and the breast is more natural when touched, and aesthetically impeccable results are obtained at a higher frequency. In the case of an asymmetrical breast, the asymmetry can be compensated by inserting a different size of implant.
A drain tube is inserted into the surgical area after surgery to drain the fluid (seroma) formed.
Drain tube removed after 1-2 days, stay in hospital is recommended. Welds may be removed after two weeks.
After surgery, the breasts (surgical area) must always be temporarily retired (most often with a special brassier or possibly with a simple soft, elastic brassier).
After sewing, it is recommended to massage the implant regularly and to move it according to the given instructions. The implant will reach its final position after about 3-4 months. Appropriate handling of the implants is very important for the development of the final breast form. This must be carried out for 6 months (one to two times a day) at the patient’s home with sufficient regularity. The wearing of stiffening brassieres is strictly forbidden for 4 months after surgery because it may lead to stuffing. In some cases, when a movement of the implant is detected, it may be necessary to wear a brassière.
It is not recommended to drive a car for at least 2 weeks after surgery, or to avoid a gymnastics for 6 weeks (middle movement that makes heavy use of the thoracic muscle).Treatment of surgical scars with silicone cream or tapas after welding is recommended, or laser treatment is recommended to achieve aesthetically impeccable scars. Sunshine and sunbeds are not recommended during this time.