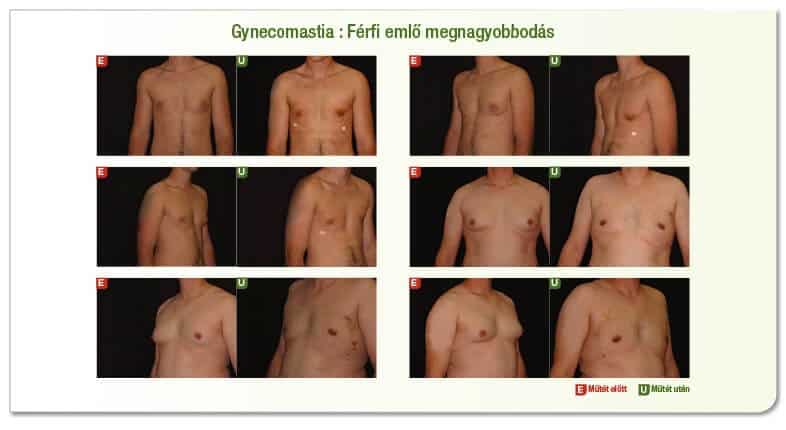
Male breast enlargement correction
The male breast is enlarged and turned into a feminine form, known as gynecomastia. It usually starts in adolescence and may be caused by hormonal lesions, steroid hormones used at a later age, or by taking various rodents. Although patients present themselves for surgery mainly because of formal deformity, it is absolutely necessary before this can be done to: endocrinological investigation to clarify hormonal relationships. The male breast consists of a small gland population, similar to a larger flat disc, with suctionous connective tissue hedges. The glands pass through the thorax wall without a sharp border into the fat tissue that spreads along the edges. Adipose tissue growth can be eliminated by grease extraction, but hardy glands can only be removed sharply by surgery. Shrinkage of the skin is expected after surgery, reduction of the skin and lifting of the udder are rarely needed. The skin is reduced in a circular way. As the scars on the chest wall can be very confusing, we try to operate with as little visible scars as possible. Only in fully developed breasts, usually from the age of 18-20 years.
The operation is carried out after a preliminary in-depth investigation, which includes the endocrinology, mammografia or breast Uh test or other tests necessary for anaesthesia, such as the laboratory, EKG, Mrtg if necessary, or blood group + Rh test.
Surgery is carried out in general anaesthesia.
For grease extraction, the fatty tissue is infiltrated with a saline containing a vasoconstricting agent or Lokál anaesteticum.
During surgery, the entire enlarged male breast stock, the fat tissue remaining on the edges, which causes contour defects, is removed by grease extraction from a semi-circle-shaped pruning at the lower boundary of the Bumbud Court. The degree of fat absorption is determined by the thickness of the contour to be formed and of the subcutaneous fat tissue visible in the rest of the chest. The wound cavity is drained and the wound edges are laminated and the skin is closed by a one-line pruning weld. The removed sample is sent for histological examination, even if no tumours are suspected, as male breast-derived malignant tumours are of the worst-beginning type.
After the operation, a compression cloth is placed, which should be worn 24/7 for 4-6 weeks. Welds are removed after 10 to 14 days, while welding is carried out in the wound and replaced at certain times. Bathing is permitted after welding.
After welding, treatment of the scar with silicone cream or tapas is recommended, with enhanced light protection recommended in the first summer.
Sub-fusions may occur in sub-prepared and fat-suctioned areas and their absorption may be stimulated by Heparin-containing cream. When the surface is no longer sensitive to the touch, a cautious massage improves the result.
Normal life can start in 2-3 weeks with compression bonding, more severe training is recommended only in 6 weeks, depending on the complaints.